Small tile blue
maxgraft® granules
Processed allograft
For experienced oral and maxillofacial surgeons, allograft bone is the only real alternative to harvesting the patient’s own autologous bone. This helps preventing well known risks such as donor-site morbidity, infection, post-operative pain, and bone-stability loss. The excellent biological regeneration capability of maxgraft® results in a predictable clinical outcome.























|
Rehydration
The processing of maxgraft® products preserves the natural collagen content and a residual water content of <10%. Thus, a rehydration is not mandatory. However, rehydration in blood or saline solution can facilitate the handling and application of maxgraft® granules due to better sticking together.
Rehydration
The processing of maxgraft® products preserves the natural collagen content and a residual water content of <10%. Thus, a rehydration is not mandatory. However, rehydration in blood or saline solution can facilitate the handling and application of maxgraft® granules due to better sticking together.
Rehydration
The processing of maxgraft® products preserves the natural collagen content and a residual water content of <10%. Thus, a rehydration is not mandatory. However, rehydration in blood or saline solution can facilitate the handling and application of maxgraft® granules due to better sticking together.
Rehydration
The processing of maxgraft® products preserves the natural collagen content and a residual water content of <10%. Thus, a rehydration is not mandatory. However, rehydration in blood or saline solution can facilitate the handling and application of maxgraft® granules due to better sticking together.
Rehydration
The processing of maxgraft® products preserves the natural collagen content and a residual water content of <10%. Thus, a rehydration is not mandatory. However, rehydration in blood or saline solution can facilitate the handling and application of maxgraft® granules due to better sticking together.
Rehydration
The processing of maxgraft® products preserves the natural collagen content and a residual water content of <10%. Thus, a rehydration is not mandatory. However, rehydration in blood or saline solution can facilitate the handling and application of maxgraft® granules due to better sticking together.
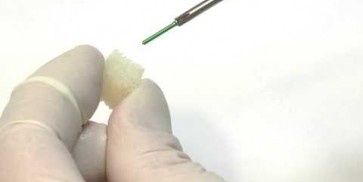
Particle application
Avoid compressing the particles excessively during application; less packed particles leave more space for blood vessel ingrowth and formation of new bone matrix.
Particle application
Avoid compressing the particles excessively during application; less packed particles leave more space for blood vessel ingrowth and formation of new bone matrix.
Particle application
Avoid compressing the particles excessively during application; less packed particles leave more space for blood vessel ingrowth and formation of new bone matrix.
Particle application
Avoid compressing the particles excessively during application; less packed particles leave more space for blood vessel ingrowth and formation of new bone matrix.
Particle application
Avoid compressing the particles excessively during application; less packed particles leave more space for blood vessel ingrowth and formation of new bone matrix.
Particle application
Avoid compressing the particles excessively during application; less packed particles leave more space for blood vessel ingrowth and formation of new bone matrix.
Mixing with autologous bone
Mixing of maxgraft® granules with autologous bone adds a biological activity (osteoinductive and osteogenetic properties of autologous bone) and supports faster regeneration and formation of new bone.
Mixing with autologous bone
Mixing of maxgraft® granules with autologous bone adds a biological activity (osteoinductive and osteogenetic properties of autologous bone) and supports faster regeneration and formation of new bone.
Mixing with autologous bone
Mixing of maxgraft® granules with autologous bone adds a biological activity (osteoinductive and osteogenetic properties of autologous bone) and supports faster regeneration and formation of new bone.
Mixing with autologous bone
Mixing of maxgraft® granules with autologous bone adds a biological activity (osteoinductive and osteogenetic properties of autologous bone) and supports faster regeneration and formation of new bone.
Mixing with autologous bone
Mixing of maxgraft® granules with autologous bone adds a biological activity (osteoinductive and osteogenetic properties of autologous bone) and supports faster regeneration and formation of new bone.
Mixing with autologous bone
Mixing of maxgraft® granules with autologous bone adds a biological activity (osteoinductive and osteogenetic properties of autologous bone) and supports faster regeneration and formation of new bone.
Mixing with cerabone®
Mixing of maxgraft® granules with xenogenic materials (cerabone®) combines the advantages of both materials; the biological potential of maxgraft® and the long-term volume stability of cerabone® lead to fast regeneration of strong vital bone.
Mixing with cerabone®
Mixing of maxgraft® granules with xenogenic materials (cerabone®) combines the advantages of both materials; the biological potential of maxgraft® and the long-term volume stability of cerabone® lead to fast regeneration of strong vital bone.
Mixing with cerabone®
Mixing of maxgraft® granules with xenogenic materials (cerabone®) combines the advantages of both materials; the biological potential of maxgraft® and the long-term volume stability of cerabone® lead to fast regeneration of strong vital bone.
Mixing with cerabone®
Mixing of maxgraft® granules with xenogenic materials (cerabone®) combines the advantages of both materials; the biological potential of maxgraft® and the long-term volume stability of cerabone® lead to fast regeneration of strong vital bone.
Mixing with cerabone®
Mixing of maxgraft® granules with xenogenic materials (cerabone®) combines the advantages of both materials; the biological potential of maxgraft® and the long-term volume stability of cerabone® lead to fast regeneration of strong vital bone.
Mixing with cerabone®
Mixing of maxgraft® granules with xenogenic materials (cerabone®) combines the advantages of both materials; the biological potential of maxgraft® and the long-term volume stability of cerabone® lead to fast regeneration of strong vital bone.
Re-entry
Depending on the defect size, the graft will be incorporated stable within 3-4 months (usage of maxgraft® granules in socket preservation, smaller bone defects, periodontal defects).
Re-entry
Depending on the defect size, the graft will be incorporated stable within 3-4 months (usage of maxgraft® granules in socket preservation, smaller bone defects, periodontal defects).
Re-entry
Depending on the defect size, the graft will be incorporated stable within 3-4 months (usage of maxgraft® granules in socket preservation, smaller bone defects, periodontal defects).
Re-entry
Depending on the defect size, the graft will be incorporated stable within 3-4 months (usage of maxgraft® granules in socket preservation, smaller bone defects, periodontal defects).
Re-entry
Depending on the defect size, the graft will be incorporated stable within 3-4 months (usage of maxgraft® granules in socket preservation, smaller bone defects, periodontal defects).
Re-entry
Depending on the defect size, the graft will be incorporated stable within 3-4 months (usage of maxgraft® granules in socket preservation, smaller bone defects, periodontal defects).

Baseline clinical situation.

Situation before extraction of the teeth

Initial clinical situation

Initial situation after extraction of tooth 21 after 6 months

Preparation of a single tooth defect with severely resorbed vestibular wall

Initial clinical situation.


Initial clinical situation


Tooth 16 furcation involvement with gingival marginal recession and large Class 5 filling

Initial x-ray, ten years post implantationem alio loco, large peri-implant bone loss

Extraction socket with bone wall defect

Situation before tooth extraction

Initial clinical situation


Initial X-ray presenting a very deep intrabony defect of tooth 21

Implant placed in the deficient site. permamem® in place for covering.

Initial situation – Treatment plan: Replace the adhesive upper left central incisor bridge with a dental implant

Occlusal view of attached maxgraft® cortico at the buccal site

Initial x-ray, tooth 25 compromised and to be extracted

Clinical situation at baseline: Situation after tooth extraction UR1 due to a failed endodontic treatment 3 months previously

Alveolar socket before soft and hard tissue augmentation

Pre-operative situation; tooth 21 proved not to be worth preserving




Initial clinical situation: 9 mm pocket depth associated with root fracture

Initial situation - A young female 34 years old lost her front teeth in an surfing accident and she had a 5 unit bridge supported by her upper left lateral and right canine. The restoration failed and both supporting crowns have exposed and leaking margins.

Initial situation - endodontically failing tooth 22, very thin biotype, high lip line and esthetic expectations

Preoperative x-ray, severe bone atrophy

Initial situation - broken and missing upper right central incisor (UR1). This tooth was removed long time ago and there were signs of bone loss and resorption due to the bone remodelling. Patient was also undergoing orthodontic treatment due to the loss of mesio-distal space.
[1] Tilaveridis I. et al, The use of mineralized bone allograft (C+TBA) as a single grafting material in maxillary sinus lifting with severely atrophied alveolar ridge (1–3mm) and immediately inserted dental implants. A 3- up to 8-year retrospective study, 2018 Oral and Maxillofacial Surgery, Sep;22(3):267-273.
[2] Simonpieri A. et al. Four-year post-loading results of full-arch rehabilitation with immediate placement and immediate loading implants: A retrospective controlled study. Quintessence Int. 2017;48(4):315-324.
maxgraft® blocks
Processed allograft
For experienced oral and maxillofacial surgeons, allograft bone blocks for block augmentation are the only real alternative to harvesting the patient’s own autologous bone. This helps preventing well known risks such as donor-site morbidity, infection, post-operative pain, and bone-stability loss. The excellent biological regeneration capability of maxgraft® results in a predictable clinical outcome.






|
Contact to local bone
Avoid larger gaps between graft and defect, because a close contact between transplant and local bone ensures block incorporation and faster regeneration.
Contact to local bone
Avoid larger gaps between graft and defect, because a close contact between transplant and local bone ensures block incorporation and faster regeneration.
Contact to local bone
Avoid larger gaps between graft and defect, because a close contact between transplant and local bone ensures block incorporation and faster regeneration.
Contact to local bone
Avoid larger gaps between graft and defect, because a close contact between transplant and local bone ensures block incorporation and faster regeneration.
Contact to local bone
Avoid larger gaps between graft and defect, because a close contact between transplant and local bone ensures block incorporation and faster regeneration.
Contact to local bone
Avoid larger gaps between graft and defect, because a close contact between transplant and local bone ensures block incorporation and faster regeneration.
Rehydration
The processing of maxgraft® products preserves the natural collagen content and a residual water content of <10%. Thus, a rehydration is not mandatory, but it is recommended. Rehydration in saline solution results in a bit more flexibility of the block, therefore it is less prone to crumble or break and can be more easily adapted to the defect area.
Rehydration
The processing of maxgraft® products preserves the natural collagen content and a residual water content of <10%. Thus, a rehydration is not mandatory, but it is recommended. Rehydration in saline solution results in a bit more flexibility of the block, therefore it is less prone to crumble or break and can be more easily adapted to the defect area.
Rehydration
The processing of maxgraft® products preserves the natural collagen content and a residual water content of <10%. Thus, a rehydration is not mandatory, but it is recommended. Rehydration in saline solution results in a bit more flexibility of the block, therefore it is less prone to crumble or break and can be more easily adapted to the defect area.
Rehydration
The processing of maxgraft® products preserves the natural collagen content and a residual water content of <10%. Thus, a rehydration is not mandatory, but it is recommended. Rehydration in saline solution results in a bit more flexibility of the block, therefore it is less prone to crumble or break and can be more easily adapted to the defect area.
Rehydration
The processing of maxgraft® products preserves the natural collagen content and a residual water content of <10%. Thus, a rehydration is not mandatory, but it is recommended. Rehydration in saline solution results in a bit more flexibility of the block, therefore it is less prone to crumble or break and can be more easily adapted to the defect area.
Rehydration
The processing of maxgraft® products preserves the natural collagen content and a residual water content of <10%. Thus, a rehydration is not mandatory, but it is recommended. Rehydration in saline solution results in a bit more flexibility of the block, therefore it is less prone to crumble or break and can be more easily adapted to the defect area.
Combination with cerabone® oder maxresorb®
Additional void volume should be filled with particulate grafting material (e.g. cerabone® or maxresorb®) to improve the esthetic outcome and to protect the soft tissue.
Combination with cerabone® oder maxresorb®
Additional void volume should be filled with particulate grafting material (e.g. cerabone® or maxresorb®) to improve the esthetic outcome and to protect the soft tissue.
Combination with cerabone® oder maxresorb®
Additional void volume should be filled with particulate grafting material (e.g. cerabone® or maxresorb®) to improve the esthetic outcome and to protect the soft tissue.
Combination with cerabone® oder maxresorb®
Additional void volume should be filled with particulate grafting material (e.g. cerabone® or maxresorb®) to improve the esthetic outcome and to protect the soft tissue.
Combination with cerabone® oder maxresorb®
Additional void volume should be filled with particulate grafting material (e.g. cerabone® or maxresorb®) to improve the esthetic outcome and to protect the soft tissue.
Combination with cerabone® oder maxresorb®
Additional void volume should be filled with particulate grafting material (e.g. cerabone® or maxresorb®) to improve the esthetic outcome and to protect the soft tissue.
Healing time
The average healing period is about 4 months for smaller defects and 6 months for larger defects.
Healing time
The average healing period is about 4 months for smaller defects and 6 months for larger defects.
Healing time
The average healing period is about 4 months for smaller defects and 6 months for larger defects.
Healing time
The average healing period is about 4 months for smaller defects and 6 months for larger defects.
Healing time
The average healing period is about 4 months for smaller defects and 6 months for larger defects.
Healing time
The average healing period is about 4 months for smaller defects and 6 months for larger defects.
Avoiding soft tissue perforation
Use flat-headed screws for fixation and avoid sharp edges that might cause a perforation of the overlying soft tissue.
Avoiding soft tissue perforation
Use flat-headed screws for fixation and avoid sharp edges that might cause a perforation of the overlying soft tissue.
Avoiding soft tissue perforation
Use flat-headed screws for fixation and avoid sharp edges that might cause a perforation of the overlying soft tissue.
Avoiding soft tissue perforation
Use flat-headed screws for fixation and avoid sharp edges that might cause a perforation of the overlying soft tissue.
Avoiding soft tissue perforation
Use flat-headed screws for fixation and avoid sharp edges that might cause a perforation of the overlying soft tissue.
Avoiding soft tissue perforation
Use flat-headed screws for fixation and avoid sharp edges that might cause a perforation of the overlying soft tissue.

Initial situation with severe maxillary atrophy

Initial situation - bone defect in maxilla after loosing right canine
Initial situation – Treatment plan: Replace the adhesive upper left central incisor bridge with a dental implant

Initial situation: 40 year old female patient with extensive scar tissue after several surgeries restored with a Rochette bridge

Initial situation before surgery. Patient lost central incisors 1 month ago due to endodontic failures

Initial CBCT scan - Fracture of left maxillary incisor and loss of buccal wall

Free-end situation in right mandible

Initial situation displaying insufficient bone width
Please Contact us for Literature.
Jason® membrane
Native pericardium membrane for GBR/GTR
Due to the unique production process, the superior properties of the native pericardium are preserved during the extensive cleaning procedure that is applied for the production of Jason® membrane. Therefore, Jason® membrane shows a natural honeycomb-like, multilayered collagen structure with an increased content of collagen type III leading to a remarkable tear resistance to and a slow degradation of Jason® membrane. This ensures a natural long barrier function, making the Jason® membrane our recommended choice particularly for large augmentative procedures.









|
Rehydration
The Jason® membrane can be applied dry or pre-hydrated in sterile saline solution or blood from the defect. The initial placement of the dry membrane with subsequent application of the graft material is particularly advantageous for lateral augmentations. After rehydration the membrane can be folded over the defect.
Rehydration
The Jason® membrane can be applied dry or pre-hydrated in sterile saline solution or blood from the defect. The initial placement of the dry membrane with subsequent application of the graft material is particularly advantageous for lateral augmentations. After rehydration the membrane can be folded over the defect.
Rehydration
The Jason® membrane can be applied dry or pre-hydrated in sterile saline solution or blood from the defect. The initial placement of the dry membrane with subsequent application of the graft material is particularly advantageous for lateral augmentations. After rehydration the membrane can be folded over the defect.
Rehydration
The Jason® membrane can be applied dry or pre-hydrated in sterile saline solution or blood from the defect. The initial placement of the dry membrane with subsequent application of the graft material is particularly advantageous for lateral augmentations. After rehydration the membrane can be folded over the defect.
Rehydration
The Jason® membrane can be applied dry or pre-hydrated in sterile saline solution or blood from the defect. The initial placement of the dry membrane with subsequent application of the graft material is particularly advantageous for lateral augmentations. After rehydration the membrane can be folded over the defect.
Rehydration
The Jason® membrane can be applied dry or pre-hydrated in sterile saline solution or blood from the defect. The initial placement of the dry membrane with subsequent application of the graft material is particularly advantageous for lateral augmentations. After rehydration the membrane can be folded over the defect.
Fixation
Jason® membrane exhibits a remarkable multi-directional tear resistance. Therefore, it can easily be pinned, sutured or even screwed without rupturing.
Fixation
Jason® membrane exhibits a remarkable multi-directional tear resistance. Therefore, it can easily be pinned, sutured or even screwed without rupturing.
Fixation
Jason® membrane exhibits a remarkable multi-directional tear resistance. Therefore, it can easily be pinned, sutured or even screwed without rupturing.
Fixation
Jason® membrane exhibits a remarkable multi-directional tear resistance. Therefore, it can easily be pinned, sutured or even screwed without rupturing.
Fixation
Jason® membrane exhibits a remarkable multi-directional tear resistance. Therefore, it can easily be pinned, sutured or even screwed without rupturing.
Fixation
Jason® membrane exhibits a remarkable multi-directional tear resistance. Therefore, it can easily be pinned, sutured or even screwed without rupturing.
Exposure
Exposure of Jason® membrane should be avoided, since fast bacterial resorption significantly reduces the barrier function of the thin Jason® membrane. In case of an unstable soft tissue situation or if you expect a wound dehiscence to occur, it is recommended to cover the membrane with a Jason® fleece (where applicable, soaked in antibiotics) to protect the healing area. In case of a dehiscence the wound usually heals without complications by formation of free granulation tissue.
Exposure
Exposure of Jason® membrane should be avoided, since fast bacterial resorption significantly reduces the barrier function of the thin Jason® membrane. In case of an unstable soft tissue situation or if you expect a wound dehiscence to occur, it is recommended to cover the membrane with a Jason® fleece (where applicable, soaked in antibiotics) to protect the healing area. In case of a dehiscence the wound usually heals without complications by formation of free granulation tissue.
Exposure
Exposure of Jason® membrane should be avoided, since fast bacterial resorption significantly reduces the barrier function of the thin Jason® membrane. In case of an unstable soft tissue situation or if you expect a wound dehiscence to occur, it is recommended to cover the membrane with a Jason® fleece (where applicable, soaked in antibiotics) to protect the healing area. In case of a dehiscence the wound usually heals without complications by formation of free granulation tissue.
Exposure
Exposure of Jason® membrane should be avoided, since fast bacterial resorption significantly reduces the barrier function of the thin Jason® membrane. In case of an unstable soft tissue situation or if you expect a wound dehiscence to occur, it is recommended to cover the membrane with a Jason® fleece (where applicable, soaked in antibiotics) to protect the healing area. In case of a dehiscence the wound usually heals without complications by formation of free granulation tissue.
Exposure
Exposure of Jason® membrane should be avoided, since fast bacterial resorption significantly reduces the barrier function of the thin Jason® membrane. In case of an unstable soft tissue situation or if you expect a wound dehiscence to occur, it is recommended to cover the membrane with a Jason® fleece (where applicable, soaked in antibiotics) to protect the healing area. In case of a dehiscence the wound usually heals without complications by formation of free granulation tissue.
Exposure
Exposure of Jason® membrane should be avoided, since fast bacterial resorption significantly reduces the barrier function of the thin Jason® membrane. In case of an unstable soft tissue situation or if you expect a wound dehiscence to occur, it is recommended to cover the membrane with a Jason® fleece (where applicable, soaked in antibiotics) to protect the healing area. In case of a dehiscence the wound usually heals without complications by formation of free granulation tissue.
Shaping
Jason® membrane can be cut to the desired shape and size with a pair of scissors - while maintaining sterility. It may be helpful to use appropriate templates for defining the required size of the membrane.
Shaping
Jason® membrane can be cut to the desired shape and size with a pair of scissors - while maintaining sterility. It may be helpful to use appropriate templates for defining the required size of the membrane.
Shaping
Jason® membrane can be cut to the desired shape and size with a pair of scissors - while maintaining sterility. It may be helpful to use appropriate templates for defining the required size of the membrane.
Shaping
Jason® membrane can be cut to the desired shape and size with a pair of scissors - while maintaining sterility. It may be helpful to use appropriate templates for defining the required size of the membrane.
Shaping
Jason® membrane can be cut to the desired shape and size with a pair of scissors - while maintaining sterility. It may be helpful to use appropriate templates for defining the required size of the membrane.
Shaping
Jason® membrane can be cut to the desired shape and size with a pair of scissors - while maintaining sterility. It may be helpful to use appropriate templates for defining the required size of the membrane.
Placement
Jason® membrane has one rough and one slightly smoother surface. The smoother, fine structured side is marked „G“ at the top right corner and should be placed towards the gingiva. The rougher side should face the bone. However, there is no problem if the membrane is placed the other way around, since the long-term barrier function of the membrane will still provide sufficient protection for the regeneration site.
Placement
Jason® membrane has one rough and one slightly smoother surface. The smoother, fine structured side is marked „G“ at the top right corner and should be placed towards the gingiva. The rougher side should face the bone. However, there is no problem if the membrane is placed the other way around, since the long-term barrier function of the membrane will still provide sufficient protection for the regeneration site.
Placement
Jason® membrane has one rough and one slightly smoother surface. The smoother, fine structured side is marked „G“ at the top right corner and should be placed towards the gingiva. The rougher side should face the bone. However, there is no problem if the membrane is placed the other way around, since the long-term barrier function of the membrane will still provide sufficient protection for the regeneration site.
Placement
Jason® membrane has one rough and one slightly smoother surface. The smoother, fine structured side is marked „G“ at the top right corner and should be placed towards the gingiva. The rougher side should face the bone. However, there is no problem if the membrane is placed the other way around, since the long-term barrier function of the membrane will still provide sufficient protection for the regeneration site.
Placement
Jason® membrane has one rough and one slightly smoother surface. The smoother, fine structured side is marked „G“ at the top right corner and should be placed towards the gingiva. The rougher side should face the bone. However, there is no problem if the membrane is placed the other way around, since the long-term barrier function of the membrane will still provide sufficient protection for the regeneration site.
Placement
Jason® membrane has one rough and one slightly smoother surface. The smoother, fine structured side is marked „G“ at the top right corner and should be placed towards the gingiva. The rougher side should face the bone. However, there is no problem if the membrane is placed the other way around, since the long-term barrier function of the membrane will still provide sufficient protection for the regeneration site.

Preoperative Ortopantomogram of the teeth planned for extraction

DVT image demonstrating horizontal and vertical amount of bone available


Extraction of tooth 21 after endodontic treatment

Implant insertion in atrophic alveolar ridge

Initial clinical situation with broken bridge abutment in regio 12 and tooth 21 not worth preserving

Initial clinical situation with gum recession and labial bone loss eight weeks following tooth extraction

Situation after tooth extraction.

Initial clinical situation
Initial situation after extraction of tooth 21 after 6 months

Situation after tooth removal.

Bone defect in area 11-21 due to two lost implants (periimplantitis) after 15 years of function

Pre-operative clinical situation: severe atrophy of the maxillary bone

60-year-old female patient presented with a chronic infection on tooth #11.
Since she has a high lip line matching the gingival margins of the adjacent central incisor and creating a root eminence is extremely important. For these reasons, the treatment of choice was an allograft bone ring enabling immediate placement of the dental implant with simultaneous regeneration of her ridge.
Initial clinical situation: 9 mm pocket depth associated with root fracture

Initial presentation of failing post retained crown with previous history of failed apicectomies and amalgam tattooing and scar tissue

Initial clinical situation with pronounced vertical and horizontal bone defect

Clinical view 8 weeks after extraction of teeth 25 and 26

Pre-operative: loss of interdental papilla between 12 and 11 associated with gingival inflammation and pus

Preoperative x-ray, multiple residual cysts of the upper jaw
Clinical situation at baseline: Situation after tooth extraction UR1 due to a failed endodontic treatment 3 months previously

Situation before extraction of the teeth

Atrophic alveolar ridge in the left mandible

Instable bridge situation with abscess formation at tooth #15 after apicoectomy

Preoperative clinical situation

Pre-operative radiographic view.

Initial situation pre-op: Central incisors with mobility 3

Initial clinical situation.

Initial situation: X-ray scan reveals eggshell thin sinus floor (1-3 mm) on both sites of the maxilla; green areas indicate the planned maxgraft® bonerings and red areas the planned implants

Pre-surgical situation. Teeth 26 and 27 missing.

Pre-op picture of affected teeth 11 and 21

Preoperative radiological situation

Clinical view of the case.

Preoperative situation – Maxillary defect in area 14-16 (loss of implant 16 due to periimplantitis, tooth 14 extracted recently and area 15 already edentulous for a while)

Initial x-ray showing bone loss around implants placed 5 years ago in another dental clinic
Initial clinical situation
Initial situation - endodontically failing tooth 22, very thin biotype, high lip line and esthetic expectations


Loss of teeth in anterior maxilla caused by periodontitis


Initial situation after root channel treatment

Preoperative CBCT analysis
Preparation of a single tooth defect with severely resorbed vestibular wall

Three implants placed in a narrow posterior mandible

Initial clinical situation with single tooth gap in regio 21

Clinical situation: 71-old patient with atrial fibrillation and Warfarin medication

Initial situation 57-year old female patient. X-ray scan reveals severe bone loss due to inflammation in region 13. Treatment plan was extraction of teeth 13 and 14 and augmentation after healing.

Initial clinical situation, regio #16

Model of the initial defect computed from a CBCT scan - buccal view

Clinical situation

Lateral view of the defect in the posterior right maxilla.


Initial clinical situation.

The patient presented with pathologic mobility of upper left central incisor. Radiographic examination revealed significant circumferential attachment loss with an unfavorable crown to root ratio.
Initial situation – Treatment plan: Replace the adhesive upper left central incisor bridge with a dental implant

Preoperative CBCT: vertical bone defects in the 3rd & 4th quadrant

Initial clinical situation: Free end situation in quadrant three and four
Initial x-ray, tooth 25 compromised and to be extracted
Preoperative x-ray, severe bone atrophy

The patient presented with severe pain in the lateral incisor and a deficient adhesive provisional. Bruxism resulted in canine loss and premature contact in the lateral incisor.
Initial x-ray, ten years post implantationem alio loco, large peri-implant bone loss
Please Contact us for Literature.
cerabone®
100% Pure bone mineral
The long-term success of cerabone® is based on its excellent osteoconductive properties and exceptional purity achieved by a unique 1200°C temperature treatment processing. The unique topographic and physico-chemical characteristics of cerabone® efficiently support blood clot formation and the proliferation of regenerative cells leading to predictable particle integration. Its non-resorbability, owing to its exceptional purity, provides stability of the augmented site on a long-term basis.

|
Rehydration
Rehydration in blood from the defect site or saline solution is not necessary but facilitates handling and application since the wetted cerabone® granules stick together.
Rehydration
Rehydration in blood from the defect site or saline solution is not necessary but facilitates handling and application since the wetted cerabone® granules stick together.
Rehydration
Rehydration in blood from the defect site or saline solution is not necessary but facilitates handling and application since the wetted cerabone® granules stick together.
Rehydration
Rehydration in blood from the defect site or saline solution is not necessary but facilitates handling and application since the wetted cerabone® granules stick together.
Rehydration
Rehydration in blood from the defect site or saline solution is not necessary but facilitates handling and application since the wetted cerabone® granules stick together.
Rehydration
Rehydration in blood from the defect site or saline solution is not necessary but facilitates handling and application since the wetted cerabone® granules stick together.
Particle compression
Avoid compressing the particles excessively during application; less packed particles leave space for blood vessel ingrowth and formation of new bone matrix.
Particle compression
Avoid compressing the particles excessively during application; less packed particles leave space for blood vessel ingrowth and formation of new bone matrix.
Particle compression
Avoid compressing the particles excessively during application; less packed particles leave space for blood vessel ingrowth and formation of new bone matrix.
Particle compression
Avoid compressing the particles excessively during application; less packed particles leave space for blood vessel ingrowth and formation of new bone matrix.
Particle compression
Avoid compressing the particles excessively during application; less packed particles leave space for blood vessel ingrowth and formation of new bone matrix.
Particle compression
Avoid compressing the particles excessively during application; less packed particles leave space for blood vessel ingrowth and formation of new bone matrix.
Healing time
A healing time of at least 6 months is recommended before re-entry to ensure stable integration of the particles.
Healing time
A healing time of at least 6 months is recommended before re-entry to ensure stable integration of the particles.
Healing time
A healing time of at least 6 months is recommended before re-entry to ensure stable integration of the particles.
Healing time
A healing time of at least 6 months is recommended before re-entry to ensure stable integration of the particles.
Healing time
A healing time of at least 6 months is recommended before re-entry to ensure stable integration of the particles.
Healing time
A healing time of at least 6 months is recommended before re-entry to ensure stable integration of the particles.
Mixing of material
Mixing of cerabone® with autologous bone bring about a biological activity (osteo-inductive and osteo-genetic properties of autologous bone) and supports faster regeneration and improved formation of new bone.
Mixing of material
Mixing of cerabone® with autologous bone bring about a biological activity (osteo-inductive and osteo-genetic properties of autologous bone) and supports faster regeneration and improved formation of new bone.
Mixing of material
Mixing of cerabone® with autologous bone bring about a biological activity (osteo-inductive and osteo-genetic properties of autologous bone) and supports faster regeneration and improved formation of new bone.
Mixing of material
Mixing of cerabone® with autologous bone bring about a biological activity (osteo-inductive and osteo-genetic properties of autologous bone) and supports faster regeneration and improved formation of new bone.
Mixing of material
Mixing of cerabone® with autologous bone bring about a biological activity (osteo-inductive and osteo-genetic properties of autologous bone) and supports faster regeneration and improved formation of new bone.
Mixing of material
Mixing of cerabone® with autologous bone bring about a biological activity (osteo-inductive and osteo-genetic properties of autologous bone) and supports faster regeneration and improved formation of new bone.

Clinical situation of the edentulous distal maxilla before the surgery

Situation before augmentation, atrophic alveolar ridge
Instable bridge situation with abscess formation at tooth #15 after apicoectomy

Clinical situation with narrow alveolar ridge in the lower jaw
Initial clinical situation with single tooth gap in regio 21

Pre-operative radiographic view.

Clinical situation before surgery

Initial situation pre-op: Central incisors with mobility 3
Situation after tooth extraction.
Initial clinical situation
Initial situation after extraction of tooth 21 after 6 months
Pre-surgical situation. Teeth 26 and 27 missing.

Pre-operative X-ray. Hopless tooth 21.

Pre-operative situation showing tooth 21 with deep periodontal pocket. Tooth presented with mobility grade III.

Initial situation: missing teeth #11 & 12 and badly broken #21 root
Preoperative radiological situation



Initial clinical situation. Atrophic maxillary ridge.

Initial clinical situation.

Initial situation with fractured central incisors
Preoperative CBCT: vertical bone defects in the 3rd & 4th quadrant
Initial clinical situation with pronounced vertical and horizontal bone defect

The patient presented with a terminal fracture of the crown tooth number 12

Initial clinical situation - Central incisors with dental destruction and periapical pathology

47 years old patient referred by another dentist after suffering a fall while fishing

Initial situation at position #16

Probing demonstrates peri-implant pocket depth of 8 mm

Situation before extraction with single tooth crowns on 21 and 22

Clinical situation before extraction and implantation
Three implants placed in a narrow posterior mandible
Preoperative clinical situation
Initial clinical situation with broken bridge abutment in regio 12 and tooth 21 not worth preserving

Pre-operative clinical situation.


Initial situation: 40 year old female patient with extensive scar tissue after several surgeries restored with a Rochette bridge
Initial situation 57-year old female patient. X-ray scan reveals severe bone loss due to inflammation in region 13. Treatment plan was extraction of teeth 13 and 14 and augmentation after healing.
Initial clinical situation.
Initial situation: X-ray scan reveals eggshell thin sinus floor (1-3 mm) on both sites of the maxilla; green areas indicate the planned maxgraft® bonerings and red areas the planned implants


Pre-operative OPG shows deep vertical intrabony defects on the distal aspects of teeth 13 and 14.

Extraction socket grafted with cerabone.

Grafting of the extraction socket with small cerabone® granules.
Lateral view of the defect in the posterior right maxilla.

Initial view of the case. Discoloration of 1.1 and mild class I gingival recession
Clinical view of the case.

The patient presented with pathologic mobility of upper left central incisor. Radiographic examination revealed significant circumferential attachment loss with an unfavorable crown to root ratio.
Initial situation – Treatment plan: Replace the adhesive upper left central incisor bridge with a dental implant
Initial presentation of failing post retained crown with previous history of failed apicectomies and amalgam tattooing and scar tissue


Initial situation with broken tooth 46
Clinical view 8 weeks after extraction of teeth 25 and 26
Initial x-ray, tooth 25 compromised and to be extracted
Preoperative x-ray, severe bone atrophy
Loss of teeth in anterior maxilla caused by periodontitis
Preoperative CBCT analysis
Atrophic alveolar ridge in the left mandible
Extraction of tooth 21 after endodontic treatment
Implant insertion in atrophic alveolar ridge

Clinical situation before augmentation

Pre-surgical probing reveals a deep intrabony defect on the distal aspect of the upper canine.

Pre-operative radiographic view. Intrabony defect on the distal aspect of the lateral incisor.

Pre-operative radiograph. Intrabony defect on the mesial aspect of tooth 14.

recession on tooth 11
Initial clinical situation with gum recession and labial bone loss eight weeks following tooth extraction

Initial clinical situation showing bone wall defect.
Initial clinical situation, regio #16

OPG of the initial situation – provision of missing denture in regio 44 to 47 by a resin-retained bridge
Situation after tooth removal.

Initial clinical situation: Bone defect in the upper right maxilla (teeth #14-16)
Pre-op picture of affected teeth 11 and 21

Initial view of the clinical case: Class III malocclusion
Treatment plan: Regenerative corticotomy (PAOO)
Initial clinical situation.

Pre-surgical situation.

Intra-operative view.

Initial clinical situation.
Initial situation - A young female 34 years old lost her front teeth in an surfing accident and she had a 5 unit bridge supported by her upper left lateral and right canine. The restoration failed and both supporting crowns have exposed and leaking margins.
Initial x-ray showing bone loss around implants placed 5 years ago in another dental clinic

Initial CBCT scan - Fracture of left maxillary incisor and loss of buccal wall

Pre-operative: loss of interdental papilla between 12 and 11 associated with gingival inflammation and pus
Preoperative x-ray, multiple residual cysts of the upper jaw
The patient presented with severe pain in the lateral incisor and a deficient adhesive provisional. Bruxism resulted in canine loss and premature contact in the lateral incisor.

Initial situation: Exposure of tooth root in position 27
[1] Tadic, D. and Epple, M. Biomaterials 2004; Vol. 25 No. 6, pp. 987–994