maxgraft® cortico
The proper size of the plate is estimated after the elevation of the mucosal flap or preoperatively using a digital planning software. Using a diamond disc, the plate is then cut extraorally. The plate is positioned within a certain distance by predrilling through the plate and local bone; fixation is performed with osteosynthesis screws to create a fixed compartment. To prevent the perforation of the soft tissue, the sharp edges have to be removed, e.g. by using a diamond ball.








|
Defect filling
To fascilitate osteosynthesis, allogenic particles (e.g. maxgraft®) can be used to fill the defect. The preserved human collagen provides excellent osteoconductivity and enables complete remodelling. Mixing with autologous chips or particulated PRF-matrizes can support the ossification.
Defect filling
To fascilitate osteosynthesis, allogenic particles (e.g. maxgraft®) can be used to fill the defect. The preserved human collagen provides excellent osteoconductivity and enables complete remodelling. Mixing with autologous chips or particulated PRF-matrizes can support the ossification.
Defect filling
To fascilitate osteosynthesis, allogenic particles (e.g. maxgraft®) can be used to fill the defect. The preserved human collagen provides excellent osteoconductivity and enables complete remodelling. Mixing with autologous chips or particulated PRF-matrizes can support the ossification.
Defect filling
To fascilitate osteosynthesis, allogenic particles (e.g. maxgraft®) can be used to fill the defect. The preserved human collagen provides excellent osteoconductivity and enables complete remodelling. Mixing with autologous chips or particulated PRF-matrizes can support the ossification.
Defect filling
To fascilitate osteosynthesis, allogenic particles (e.g. maxgraft®) can be used to fill the defect. The preserved human collagen provides excellent osteoconductivity and enables complete remodelling. Mixing with autologous chips or particulated PRF-matrizes can support the ossification.
Defect filling
To fascilitate osteosynthesis, allogenic particles (e.g. maxgraft®) can be used to fill the defect. The preserved human collagen provides excellent osteoconductivity and enables complete remodelling. Mixing with autologous chips or particulated PRF-matrizes can support the ossification.
Rehydration
Rehydration of maxgraft® cortico is recommended; Rehydration of maxgraft® cortico (10 minutes in saline solution) has been shown to increase flexibility and improve fracture strength.
Due to the composition of 100% cortical mineralized bone, significant liquid uptake is not to be expected.
Rehydration
Rehydration of maxgraft® cortico is recommended; Rehydration of maxgraft® cortico (10 minutes in saline solution) has been shown to increase flexibility and improve fracture strength.
Due to the composition of 100% cortical mineralized bone, significant liquid uptake is not to be expected.
Rehydration
Rehydration of maxgraft® cortico is recommended; Rehydration of maxgraft® cortico (10 minutes in saline solution) has been shown to increase flexibility and improve fracture strength.
Due to the composition of 100% cortical mineralized bone, significant liquid uptake is not to be expected.
Rehydration
Rehydration of maxgraft® cortico is recommended; Rehydration of maxgraft® cortico (10 minutes in saline solution) has been shown to increase flexibility and improve fracture strength.
Due to the composition of 100% cortical mineralized bone, significant liquid uptake is not to be expected.
Rehydration
Rehydration of maxgraft® cortico is recommended; Rehydration of maxgraft® cortico (10 minutes in saline solution) has been shown to increase flexibility and improve fracture strength.
Due to the composition of 100% cortical mineralized bone, significant liquid uptake is not to be expected.
Fixation
maxgraft® cortico should be positioned within a certain distance to the bone defect by predrilling through the plate and local bone, fixating with screws and therefore creating a compartment/container. The position should enable the placement of a later implant with a distance of at least 1 mm from the cortical strut. Pre-drilling is recommended. It is suggested to use a smaller diameter for the pre-drilling than the diameter of the later placed screws. Screws consisting of surgical steel with a diameter of 1.0–1.2 mm, or titanium with 1.2–1.4 mm and a length of 8–11 mm are appropriate for most defects. The use of flat-headed osteosynthesis screws is strongly recommended.
Fixation
maxgraft® cortico should be positioned within a certain distance to the bone defect by predrilling through the plate and local bone, fixating with screws and therefore creating a compartment/container. The position should enable the placement of a later implant with a distance of at least 1 mm from the cortical strut. Pre-drilling is recommended. It is suggested to use a smaller diameter for the pre-drilling than the diameter of the later placed screws. Screws consisting of surgical steel with a diameter of 1.0–1.2 mm, or titanium with 1.2–1.4 mm and a length of 8–11 mm are appropriate for most defects. The use of flat-headed osteosynthesis screws is strongly recommended.
Fixation
maxgraft® cortico should be positioned within a certain distance to the bone defect by predrilling through the plate and local bone, fixating with screws and therefore creating a compartment/container. The position should enable the placement of a later implant with a distance of at least 1 mm from the cortical strut. Pre-drilling is recommended. It is suggested to use a smaller diameter for the pre-drilling than the diameter of the later placed screws. Screws consisting of surgical steel with a diameter of 1.0–1.2 mm, or titanium with 1.2–1.4 mm and a length of 8–11 mm are appropriate for most defects. The use of flat-headed osteosynthesis screws is strongly recommended.
Fixation
maxgraft® cortico should be positioned within a certain distance to the bone defect by predrilling through the plate and local bone, fixating with screws and therefore creating a compartment/container. The position should enable the placement of a later implant with a distance of at least 1 mm from the cortical strut. Pre-drilling is recommended. It is suggested to use a smaller diameter for the pre-drilling than the diameter of the later placed screws. Screws consisting of surgical steel with a diameter of 1.0–1.2 mm, or titanium with 1.2–1.4 mm and a length of 8–11 mm are appropriate for most defects. The use of flat-headed osteosynthesis screws is strongly recommended.
Fixation
maxgraft® cortico should be positioned within a certain distance to the bone defect by predrilling through the plate and local bone, fixating with screws and therefore creating a compartment/container. The position should enable the placement of a later implant with a distance of at least 1 mm from the cortical strut. Pre-drilling is recommended. It is suggested to use a smaller diameter for the pre-drilling than the diameter of the later placed screws. Screws consisting of surgical steel with a diameter of 1.0–1.2 mm, or titanium with 1.2–1.4 mm and a length of 8–11 mm are appropriate for most defects. The use of flat-headed osteosynthesis screws is strongly recommended.
Flexibility
maxgraft® cortico cannot be bent to follow the ridge contour. It is fully mineralized cortical bone and not flexible. Cutting of the strut can be performed using the cortico trimmer. For the incisor region, it is advised to cut the strut in the middle and fixate the two parts to form the ridge contour.
Flexibility
maxgraft® cortico cannot be bent to follow the ridge contour. It is fully mineralized cortical bone and not flexible. Cutting of the strut can be performed using the cortico trimmer. For the incisor region, it is advised to cut the strut in the middle and fixate the two parts to form the ridge contour.
Flexibility
maxgraft® cortico cannot be bent to follow the ridge contour. It is fully mineralized cortical bone and not flexible. Cutting of the strut can be performed using the cortico trimmer. For the incisor region, it is advised to cut the strut in the middle and fixate the two parts to form the ridge contour.
Flexibility
maxgraft® cortico cannot be bent to follow the ridge contour. It is fully mineralized cortical bone and not flexible. Cutting of the strut can be performed using the cortico trimmer. For the incisor region, it is advised to cut the strut in the middle and fixate the two parts to form the ridge contour.
Flexibility
maxgraft® cortico cannot be bent to follow the ridge contour. It is fully mineralized cortical bone and not flexible. Cutting of the strut can be performed using the cortico trimmer. For the incisor region, it is advised to cut the strut in the middle and fixate the two parts to form the ridge contour.

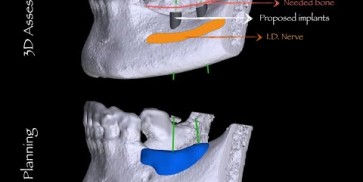
Preparation of a single tooth defect with severely resorbed vestibular wall

Model of the initial defect computed from a CBCT scan - buccal view

Severe atrophy of the ridge

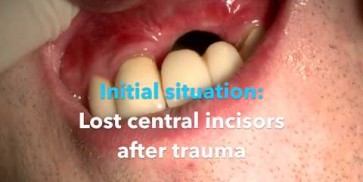
Initial clinical situation

Initial clinical situation – missing bonein regio 11, 12, 21, 22 and scarred soft tissue

Clinical situation


Occlusal view of attached maxgraft® cortico at the buccal site

OPG of the initial situation – provision of missing denture in regio 44 to 47 by a resin-retained bridge

Clinical situation

Preoperative CBCT: vertical bone defects in the 3rd & 4th quadrant
Please Contact us for Literature.